Anyone who has spent time with children knows that Kids Say The Darndest Things. This is so widely understood that many TV programs exploit it for laughs. Kids will often repeat a phrase they have heard out of context, or confidently assert an idea that they clearly don’t understand, and in some circumstances this can be hilarious.
That young children might be unreliable narrators, becomes a much more serious issue in the field of medical science. When it comes to prescribing very consequential medical interventions for kids, doctors know that the self-reporting of children must be treated with extreme caution. Many parents will have experience of what this means in practice. As part of the diagnostic process, doctors will often seek many alternative sources of information other than the self-reporting of a child. This frequently includes reports from extended family or school teachers, and interviews with parents while the child is not present. Even when talking directly with a child, doctors will often prioritise their own clinical judgement over the plain meaning of the words that a child may use.
The fact that the self-reporting of say an 11 year-old child may be unreliable, was one of the motivations for the tweet illustrated below.
This question related to a gender dysphoric 11 year-old being given puberty blockers, with a promise that cross-sex hormones would follow shortly thereafter. We know that very many perfectly healthy gay adults report having experienced gender dysphoria when they were that age. Most people who have suffered distress from such dysphoria simply grew out of it, such that administering life-altering drugs to treat the condition would have been a terrible mistake. In this context, it makes sense to ask how can we distinguish those 11 year-olds who will benefit from puberty blockers and cross sex hormones, from the children who will otherwise grow up to be a healthy young adult in just a few years.
In relation to this decision, the stakes are higher than most 11 year-olds could understand at that age. Whereas studies show that childhood gender dysphoria will naturally desist over time in a very large majority of cases, pharmaceutical interventions often leave patients sterile and suffering from other serious medical conditions. Consequently, it is not only perfectly rational to ask how we can be certain that these treatments are being prescribed for the correct patients, it is hugely important to have confidence that the prescription of life-altering drugs is appropriate for 11 year-olds who cannot self-report reliably.
In fact it is clear that this question as posed is rhetorical, since there is no widely agreed set of medical criteria to effectively determine which 11 year-olds are “trans”. Moreover, without any consensus on this topic it is inevitable that there will be significant inconsistencies in the practice of various clinicians, with the danger that gender transition interventions are applied to some children too quickly. This is exactly what happened at the Gender Identity Development Service (GIDS), which operated across the UK. Hannah Barnes is a journalist from the flagship BBC Newsnight program. She has reported how an internal GIDS audit demonstrated that their clinicians could not tell which gender dysphoric children would go on to transition as adults, and which would see their dysphoria naturally desist without any medical intervention. In the short video clip below, Hannah Barnes describes how the same question that is described in the tweet illustrated above, caused the UK government to close down GIDS.
After covering this medical scandal in detail for BBC Newsnight, Hannah Barnes wrote a book about the issue and the GIDS story has since been very widely covered across most mainstream media. As reported by the BBC and others, when the clinicians at GIDS realised that their own data showed they were prescribing “dangerous” medical interventions for gay kids, some left and became whistleblowers while others carried on. Hannah Barnes suggests two reasons that might explain why this medical scandal persisted for so long. One factor was that anyone who highlighted the problem was called a “transphobe”. Another factor was that some people could just not accept that they had been supporting something that was causing real harm to very many vulnerable children.
Following the medical scandal at GIDS, the use of puberty blockers for gender dysphoric children in the UK is now restricted to clinical research only. Many other countries have also introduced similar prohibitions on the use of puberty blockers. However, a straightforward question about how suggestible 11 year-olds might be, has demonstrated that the factors which permitted the GIDS medical scandal to persist for so long have certainly not gone away.
The sections below describe several increasingly deranged reasons for persisting with medical interventions for some 11 year-olds, in the face of so much evidence that many vulnerable children are suffering serious harms.
“Self-Reporting Is Science”
Richard Feynman gave us one of the most famous elucidations of the scientific method when he explained that, “the first principle is that you must not fool yourself and you are the easiest person to fool”. Whereas some self-professed rationalists will rightly insist that this principle must apply to even the most talented scientists in their field, the same people will create exceptions for a distressed 11 year-old child. When the context is an 11 year-old who presents as being confused about their gender, then we are told that “self-reporting is science”. In fact, it is difficult to imagine a more fundamental misunderstanding of medical science than this quote, which is taken from the thread illustrated above.
The same self-professed rationalists who will laugh heartily at a statement like, “my mind or spirit was placed in this body by my creator”; will somehow insist on the utmost reverence for a statement like, “my mind or spirit was born in the wrong body”. Some kids may make statements like this in a slightly echolalic manner, whereas others may be expressing genuine distress about these issues. Of course, any child suffering from gender dysphoria deserves the utmost compassion and care according to the best medical evidence. However, slogans like “self-reporting is science” serve only to perpetuate an ideology and do not serve the best interests of vulnerable children.
Comparisons To Mental Disorders
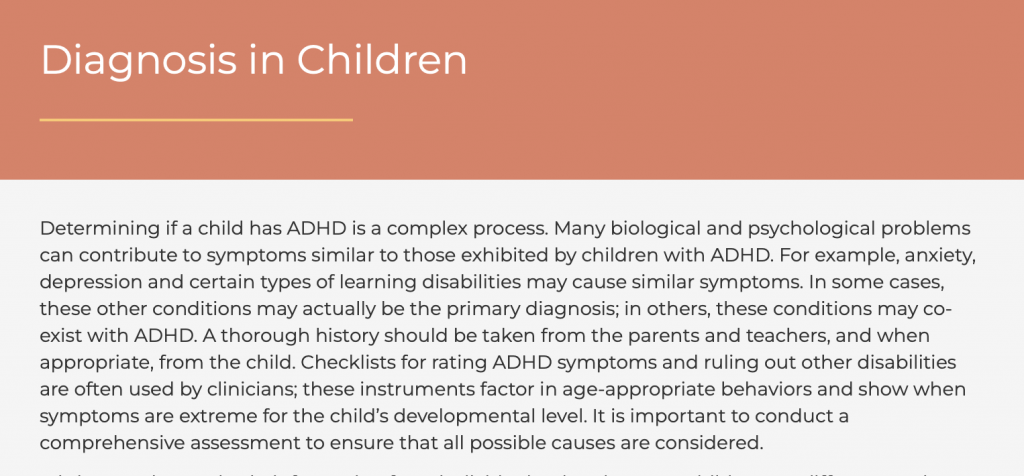
The same people who insisted that “self-reporting is science” in the thread illustrated above, also compared pharmaceutical interventions for gender dysphoria to prescribing drugs for children with mental disorders. It was proposed that the treatment of childhood mental disorders involves administering various drugs on a “trial and error” basis, and then adjusting the drug prescriptions based on the “self-reporting” of the child. This is simply not true. In fact, for any childhood mental disorder (such as ADHD) doctors will work through many steps in order to rule out comorbidities, by gathering information from sources other than the self-reporting of a paediatric patient.
In fact, not only is child self-reporting considered unreliable when diagnosing complex medical conditions, a child’s reporting of their own outcomes from their own treatment is also considered unreliable.
“Despite recent advances in child patient reported outcome assessment, barriers to the widespread use of child-report measurement tools remain. Developmentally normative variation in the cognitive capacities needed to accurately self-report, which is especially pronounced in middle childhood, makes it difficult for end-users to determine whether they should administer patient reported outcome measures to a child and once data are collected, whether they accurately reflect a child’s true health state … ‘content responsive faking’ assumes that respondents understand questions and alter their responses for gain (for example, to avoid punishment). Such measures may be problematic for children, because they are often administered by people in positions of power. Even when patient reported outcome measures have no direct bearing on children, they may misunderstand the potential consequences of the measures and intentionally alter their responses accordingly.”
Quote from a review of studies on child self-reporting among 8-11 year-olds
Most parents will read language like this in a scientific paper and roll their eyes at a conclusion that states the blindingly obvious. Of course 11 year-olds will often repeat things they have heard without fully understanding the ideas they are expressing. Of course 11 year-olds will often tell adults what they think those adults will want to hear. Of course 11 year-olds will often be suggestible. It is utterly bizarre that some people will insist that for an 11 year-old, “self-reporting is science”. It is even more absurd that this only seems to apply when the child is talking about one topic in particular. This is ideology and not medical care.
Wrong To Question In Any Way
Many rationalists have noticed that when an ideology becomes impossible to defend, its adherents often resort to condemning those who question it. In the video above, Hannah Barnes described a leadership at GIDS that referred to any questions about what they were doing as “transphobic”. Of course transphobia exists, but merely condemning the questioner is not a reasonable way to evaluate whether or not 11 year-olds might be suggestible.
Consider an 11 year-old child who reports to their parent that they are definitely heterosexual. I have parented four children through that period of their lives. If such a statement were made to me, I would think that it could be accurate or that it could be a simple restatement of a comment picked up in a different context. It could be that an 11 year-old has carefully considered their own sexuality and come to a definitive conclusion, or it could be that a child who has barely begun puberty is not yet able to fully understand their own sexuality. I don’t think such a statement would be reliable coming from an 11 year-old, and this would also be true if an 11 year-old reported that they were gay or bisexual. Kids have plenty of time to figure this out, and there is no need to treat everything that an 11 year-old says as immediately infallible.
Nevertheless, it seems that any failure to revere such a statement made by an 11 year-old child can be extrapolated to convict people of many serious transgressions.
The statement being discussed here is that an 11 year-old child might say something about sexuality that they don’t yet fully understand. This is an extraordinary series of abusive bigotries to convict a parent of, merely for considering the various different reasons why their young child might make a comment about complex issues. However, sometimes justifying an ideology requires imagining that anyone who doesn’t share it must be evil.
Many psychologists believe that projection is a defence mechanism for those suffering cognitive dissonance. For example, someone who thinks of themselves as a good person may suffer distress if they are given evidence that they have been supporting a policy which harms children. One response to this distress might be to imagine that the person who provided the evidence is harming their own children.
Denial Of Reality
Many rationalists have noticed that when an ideology is demonstrably inconsistent with reality, its adherents get busy denying reality. Sometimes this process can be witnessed in real time from one sentence to the next. Consider the short video clip below about the BBC report on GIDS, which was described above. Since there were no agreed criteria at GIDS for when life-altering drugs should be prescribed for gender dysphoric kids, many children were given unnecessary pharmaceutical interventions that caused real harm. As a result, GIDS has been closed down and replaced with two new clinics, both of which are explicitly prohibited from prescribing puberty blockers outside of clinical research. Watching the clip below, it’s amazing how the human mind can clearly absorb the specific details of this story, and then within a few sentences begin denying the reality of those same details.
The progression of their statements over a couple of minutes was as follows:
- “patients were referred onto a gender transitioning pathway too quickly”
- “the treatment or care should stop”
- “there were whistleblowers, that’s a good thing”
- “they are opening two new clinics to make the sustainability better”
- “they are not idiots and they know what they’re doing”
- “the system is operating as intended”
- “if the issue was trans children getting care they shouldn’t be getting, then they wouldn’t be opening two more facilities”
- “they are continuing the care for thousands of children”
After recognising that gender transition interventions had improperly been prescribed for many children, they initially welcomed the whistleblowing that brought an end to this incredibly harmful medical scandal. Within a few sentences though, they were welcoming the idea that this “care” might be applied to even more children by doubling the number of clinics. That is, they read aloud a BBC report about the government closing down GIDS and banning the kind of “care” that GIDS had provided, but by the end of the report they had convinced themselves that the story was really about this “care” being greatly expanded.
The Bigotry Of Punctuation
Whereas there could hardly be a more serious topic than medical scandals which harm children, some of the responses are undeniably hilarious. The original question had put the term “trans” in quotation marks when discussing the prescription of puberty blockers for an 11 year-old child. I did the same thing because even the most experienced clinicians can’t tell which gender dysphoric 11 year-olds will observe their distress desist, and which will be happier as adults after having transitioned.
However, the “self-reporting is science” crowd who insist that any 11 year-old child is definitely “trans” if they merely say that they are “trans”, can be driven somewhat loopy by punctuation.
This contribution was no more deranged than any of the rest of it but at least it ended up being pretty funny, if not for the reasons intended.
3 responses to “How Suggestible Are 11 Year-Olds?”
https://youtube.com/live/Pokt739WlFo?feature=share
[…] a recent discussion on the treatment of 11 year-old children who are suffering from gender dysphoria, I was told that “tighty whities have a greater effect on fertility than puberty […]
[…] response is to affirm whatever the child is reporting about their own sexuality. Conversely, I had written a previous article arguing that because 11 year-olds can be suggestible, merely using words like “trans” […]