Some months ago I wrote an article about the interim Cass Report, in which I summarised the findings with detailed references to the document itself. Dr Hilary Cass had been conducting an independent review of the Gender Identity Development Service (GIDS) in the UK. Following her interim report it was announced that GIDS was to be closed down, as Dr Cass had concluded that persisting with that approach was “not a safe or viable long-term option”. This week, it has been reported that new training on a very different service to replace GIDS has been delayed. This is in part because of the significant changes that will be made to the nature of the care that was provided to vulnerable children by GIDS.
The actual conclusions of the interim Cass Report into GIDS were as follows:
- The clinicians at GIDS could not agree on the nature of the gender dysphoria disorders that they were treating.
- The clinicians at GIDS had no agreed set of criteria to determine which gender dysphoric children would observe their distress desist naturally, and which would retain a stable transgender identity throughout adulthood.
- Many young children were prescribed puberty blockers very quickly (perhaps after just two consultations) and 98% of those prescribed puberty blockers remained on a treatment pathway that progressed through years of cross-sex hormones.
- Among the clinicians at GIDS themselves, there was concern about a high number of “false positives” whereby children who would otherwise have grown up to be healthy gay adults were instead prescribed life-altering treatments.
The interim Cass Report also included a survey of the international research in this area. As a result, there can be confidence that the best available scientific evidence demonstrates the following:
- The majority of gender dysphoric children come to realise during puberty that they are gay, which typically resolves the distress that they had been experiencing.
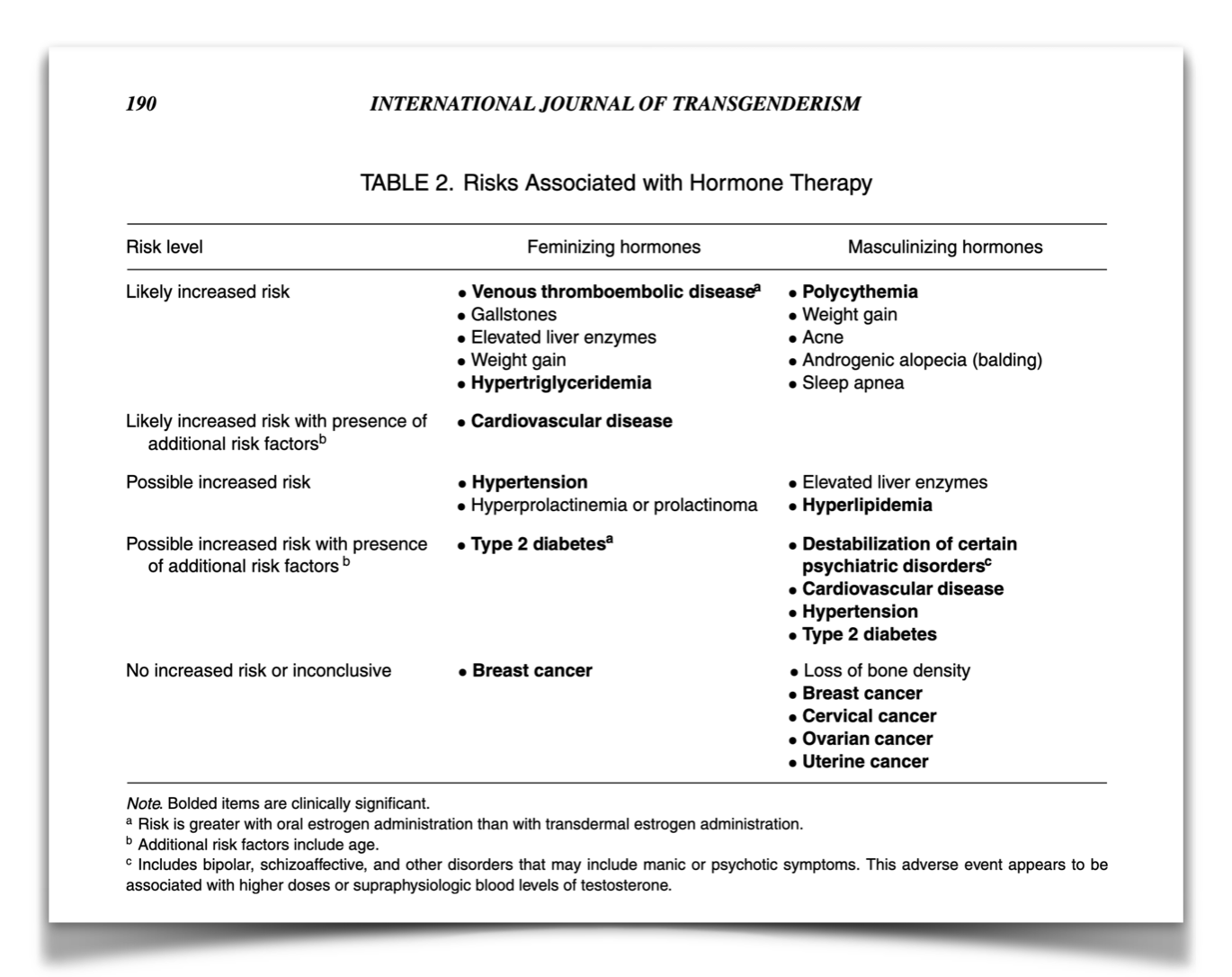
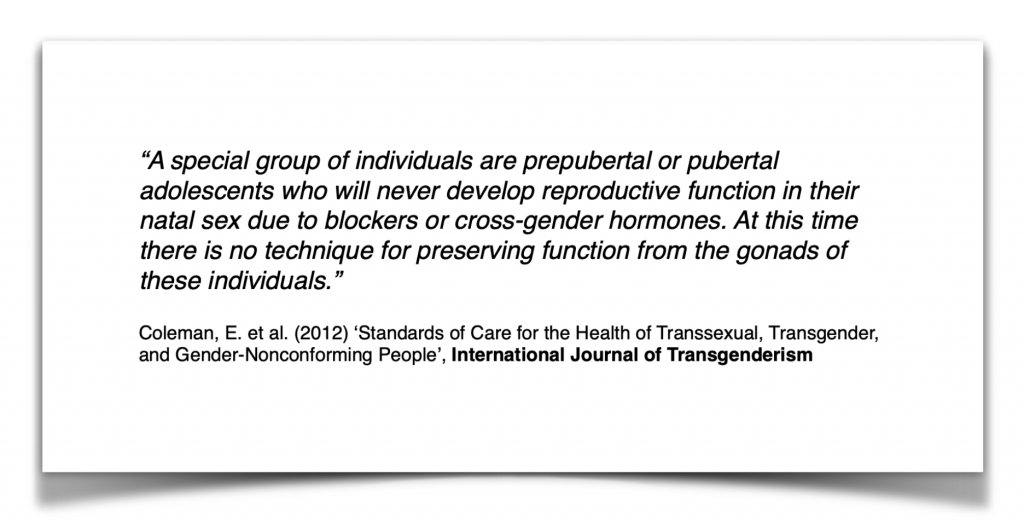
- The treatment pathway that was being prescribed at GIDS, beginning with puberty blockers for young children, often causes sterilisation and other life-altering clinically relevant conditions.
{kind=link}
In fact, we didn’t really need peer-reviewed scientific research to tell us any of this. It was already common knowledge that most gender dysphoric kids realise during puberty that they are gay, such that their dysphoria desists without pharmaceutical intervention. That is, in the majority of such cases puberty is the cure for gender dysphoria and blocking puberty is counter-productive. Moreover, if a prepubescent child has their puberty blocked until their late teens such that they can never subsequently undergo the physical developments associated with puberty, then of course they may never become fertile.
In other words, when clinicians refer to “false positives” at services like GIDS, they are really employing a euphemism for the entirely unnecessary chemical sterilisation of gay children. In fact, there had been internal whistleblowers (and some external commentators) who had drawn attention to the child safeguarding dangers associated with these “false positive” cases. This is why the National Health Service (NHS) in England decided to close down GIDS following the interim Cass Report. They also introduced strict new prohibitions on the prescription of the treatment pathway that GIDS had placed many vulnerable children onto. This is also why the Irish clinicians with the most experience in this area raised their own concerns about the gender-affirming treatment pathway at GIDS.
Whereas it has already been announced that GIDS is to be closed down, it is important to consider how the GIDS assessment and treatment model could have persisted for so long, when the harms being caused to vulnerable children were so clear. Why were the child safeguarding concerns of internal clinical whistleblowers not actioned? Why wasn’t the volume of critical commentary so overwhelming as to ensure the protection of vulnerable children? Hannah Barnes is a BBC journalist who interviewed many clinicians, administrators and patients at GIDS. She has reported that one reason for the persistence of this medical scandal, was that anyone who expressed any apprehension about what GIDS was doing was labelled a transphobic bigot.
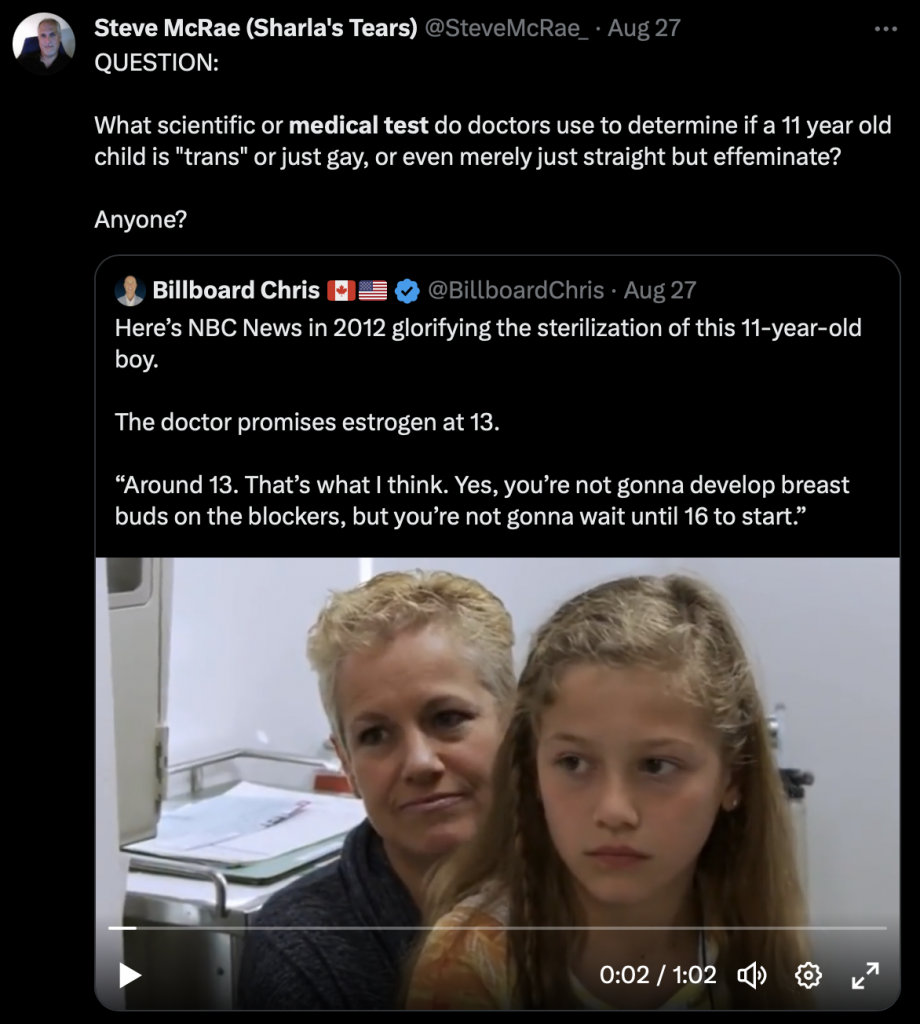
Undoubtedly, one reason why the GIDS treatment pathway continued causing harm to vulnerable children for so long, was the virulence of the online mobs screaming “transphobe” at anyone who expressed any concern. In fact the minor examples of this that I have seen are of course only a tiny fraction of the appalling vituperation directed at clinician whistleblowers and prominent commentators. Nevertheless, it would not be fair or reasonable to point to any one tweet; or any one video; or any one podcast; from any one person; and state that any single online comment caused harm to children. However, the overall environment created by the online mobs most certainly did prolong a lot of very real harm that was caused to very many distressed children, and we can usefully observe who was willing to join the pile ons. It is worth noticing which people were eager to ignore easily demonstrable objective facts, and enthusiastically adopt ideas so absurd that they would shame the most preposterous Q-Anon cultists, all so that they could fling false allegations at anyone highlighting a very real child safeguarding issue.
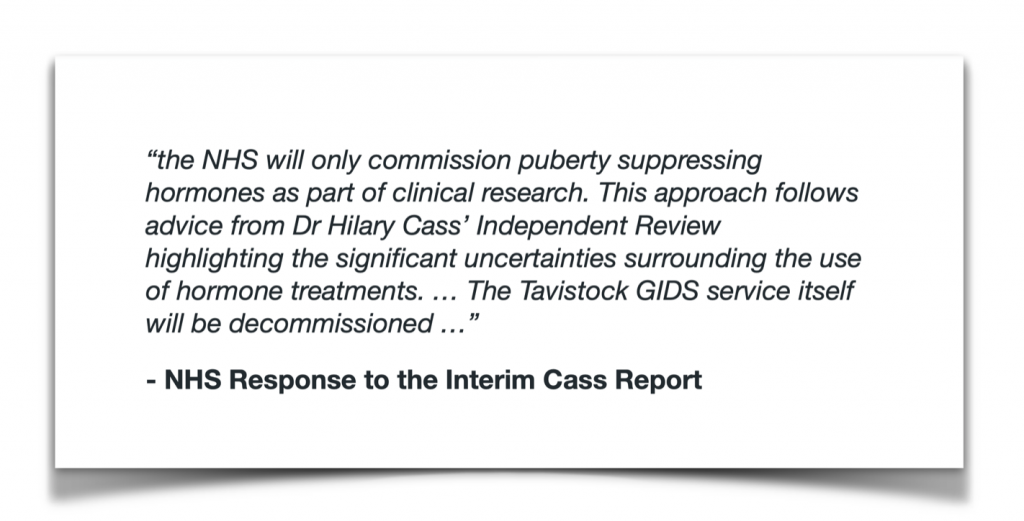
Ideologues like Q-Anon cultists and others, can convince themselves of the most risible un-evidenced ideas in order to preserve their pet theories. The video clip above describes an example of one such deranged delusion, which cannot pass the laugh test. Whereas the immediate NHS response to the interim Cass Report was to close down GIDS and prohibit the prescription of any further puberty blockers outside of clinical research, the idea advanced in this video clip is that the NHS decommissioned GIDS in order to prescribe more puberty blockers to more children. GIDS operated a number of clinics in various cities around England. If as claimed in this video clip the only problem described in the Cass Report was long waiting lists, then why would the NHS close down GIDS? Why would they not just add some more clinics to GIDS wherever in England the excess demand was located?
In her latest reporting, Hannah Barnes has described as follows the delay in creating the new training required in order to replace GIDS:
“Cass called for a “fundamentally different” approach under which young people’s other difficulties are considered alongside their gender-related distress, and different children could receive different treatments. The NHS plans that puberty blockers, a referral for which was routine practice at GIDS, will only be made available as part of a clinical research trial or in exceptional cases … NHS England’s official position remains that the first two new services will be fully mobilised in April 2024. But given no training of staff has taken place, and that the content of that training hasn’t even been written yet, it seems highly unlikely. Another option might be that a small number of staff are trained initially, with capacity gradually built up. Young people have been badly let down by the NHS. But there will not be another opportunity to get youth gender services right. If that takes a few more months, maybe the short-term pain will be worthwhile.”
Hannah Barnes writing in The New Statesman
It is astounding that in order to convince themselves that there were no child safeguarding concerns with the GIDS treatment pathway, some people have managed to ignore the fact that the NHS decided to close down GIDS and introduce prohibitions on the prescription of puberty blockers. They instead label anyone who refers to these child safeguarding measures as a transphobic bigot. Their insistence is on ignoring all issues relating to child safeguarding, and instead maintaining a fantasy that the only reported problem was that the GIDS waiting list for puberty blockers was too long. Of course, it is utterly risible to suggest that the NHS decided to close down GIDS and introduce strict prohibitions on the prescription of puberty blockers, in order to shorten waiting lists and treat more children with more puberty blockers. Nevertheless, actual adults said this out loud; they deliberately recorded a video of themselves saying it; and then they uploaded the video to the public internet. It really is an incredible feat of self-delusion.
Of course it is true that everyone prefers shorter waiting lists to longer waiting lists. Of course the Cass Report recommended shorter waiting times before consultation, rather than longer waiting times. Of course there was no dispute whatsoever on this point. Nobody was arguing for longer waiting lists. Instead, the core issue was the nature of the treatment that those patients would receive once they began consultations. Following the recommendations of Dr Cass, the pharmaceutical treatment pathway that had so often been prescribed by GIDS, was prohibited. Q-Anon levels of conspiracy theorising are required to look at the closure of the body prescribing the puberty blockers; and to look at the new prohibitions preventing any other body from prescribing this treatment to gender dysphoric kids; and to conclude that this was all designed to get more kids onto the GIDS gender transition pathway.
Nevertheless, the cultists will not change their position now that the latest reporting has described how much re-training is required. They are as impervious to documented evidence and objective facts as the most unhinged Q-Anon adherent. Moreover, another commonality that the online mobs screaming “transphobe” share with Q-Anon cultists, is their vivid imagination about all of the transgressions that those they oppose must be guilty of. Whereas febrile Q-Anon minds created all sorts of fantasies about what was happening in the basement of pizza restaurants, the minds of some other cultists can also manufacture mythologies about people they have never met.

Some of these false allegations are of such a despicable nature that they would make anyone wonder about the minds that fabricated them. In an environment like this, the reticence that Hannah Barnes described with respect to addressing the child safeguarding issues at GIDS is not in the least surprising. Knowing the abuse that would be directed at them for reporting straightforward scientific facts about the harms being caused to vulnerable children, of course some people had second thoughts about speaking out. In contrast, those who join this kind of online mob often have no discernible interest whatsoever in the wellbeing of children suffering from gender dysphoria. How else could we explain a suggestion that the unnecessary sterilisation of vulnerable children is “not the end of the world” because “adoption is an option”?
People who can make such crass comments about entirely unnecessary and life-altering harms being inflicted upon gender dysphoric children, are not motivated by child safeguarding. Their only concerns are burnishing their in-group credentials, and scoring points in their ideological culture war by screaming entirely unwarranted abuse at others. They may well have gotten their dopamine hits from inventing and broadcasting the most appalling false allegations about named people, but the only effect of this behaviour was to create the environment that caused the persistence of serious harms to vulnerable children.
Recording these facts will not cause any of these people to acknowledge the falsity of their statements or to change their behaviour. No amount of careful reports by clinical professionals will convince them of the scientific facts, any more than Q-Anon adherents can be convinced by documented evidence. However, it is worth noticing who these people are for exactly the same reason that it is worth noticing who the Q-Anon cultists are. When the same people next identify a bogeyman that they want to point fingers at, it will be informative to consider how demented their previous set of allegations were.